Introduction & Background of Fibrodysplasia Ossificans Progressiva (FOP) – Muscle turns into bone
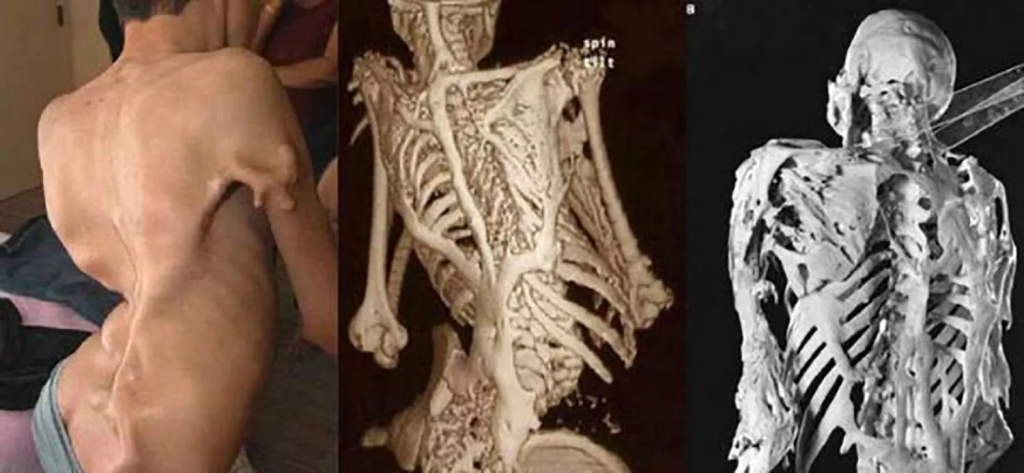
Fibrodysplasia Ossificans Progressiva (FOP) is an exceptionally rare, debilitating, and progressive genetic disorder. Often referred to as “Stone Man Syndrome,” its defining characteristic is the gradual, irreversible replacement of skeletal muscle, tendons, ligaments, and other connective tissues into heterotopic (in the wrong place) bone. This process forms a second skeleton outside the normal one, effectively locking the body in a cage of bone.
FOP is a congenital condition, meaning it is present from birth. It is estimated to affect approximately 1 in 1.4 to 2 million people worldwide, with no ethnic, racial, or gender predisposition. The condition is often misdiagnosed initially, as its early symptoms can resemble childhood cancers or other muscular conditions, leading to harmful invasive procedures. The journey of an individual with FOP is marked by progressive loss of mobility and severe physical disability.
Causes of Fibrodysplasia Ossificans Progressiva (FOP)
FOP is caused by a spontaneous mutation in the ACVR1 gene (Activin A Receptor Type I) in the vast majority of cases. This gene provides instructions for making a protein that is part of the bone morphogenetic protein (BMP) pathway, which is critical for the development and repair of the skeleton.
- The Specific Mutation: The most common mutation, known as c.617G>A; R206H, causes a single “misspelling” in the genetic code.
- The Mechanism: This faulty gene creates a hyperactive receptor that disrupts the normal BMP signaling pathway. It essentially tricks the body into forming bone in places where it shouldn’t, and at times when it shouldn’t (e.g., after minor injuries or inflammation). This process of heterotopic ossification is the central pathology of FOP.
- Inheritance Pattern: Most individuals with FOP have no family history of the disorder, as the mutation occurs spontaneously. If a person with FOP were to have children, there would be a 50% chance of passing the mutated gene to each child (autosomal dominant inheritance).
Indications of Fibrodysplasia Ossificans Progressiva (FOP)
The “indications” of FOP are the classic signs that point a clinician toward this specific diagnosis. The two most critical indications are:
- Congenital Malformations of the Great Toes: This is the most important diagnostic clue. Virtually all newborns with FOP have characteristic malformations of the big toes, which are short, bent inward (valgus deviation), and often have a monophalangic (single bone) appearance.
- Swellings or Flare-Ups: The appearance of painful, soft-tissue swellings (flare-ups) on the head, neck, or back during early childhood, which eventually transform into bone.
Symptoms of Fibrodysplasia Ossificans Progressiva (FOP)
Symptoms progress in a characteristic pattern, typically from the neck and shoulders down to the limbs and finally the jaw.
- Early Childhood: The hallmark toe malformation is present at birth. The first flare-ups often begin before age 10.
- Flare-Ups: These are episodic, inflammatory events characterized by:
- Painful, red, warm, and swollen lumps on the back, neck, or shoulders.
- These swellings can appear spontaneously or be triggered by minor trauma, viral illnesses, immunizations, or even dental work.
- Over weeks to months, these swellings resolve, leaving behind mature bone.
- Progressive Immobility: As heterotopic bone forms across joints (shoulders, elbows, hips, knees), movement becomes progressively restricted. Individuals may lose the ability to raise their arms, walk, or even open their mouth.
- Secondary Complications:
- Respiratory Failure: If heterotopic bone forms around the rib cage, it restricts lung expansion, making breathing difficult and increasing the risk of pneumonia.
- Malnutrition: Jaw locking can make eating and speaking extremely difficult.
- Hearing Loss: Some individuals experience conductive hearing loss.
- Scoliosis: Abnormal curvature of the spine is common.
Prevention Strategies of Fibrodysplasia Ossificans Progressiva (FOP)
There is no way to prevent the genetic mutation that causes FOP. Therefore, prevention strategies focus entirely on avoiding activities and procedures that could trigger flare-ups and new bone formation.
- Avoid Trauma: Prevent falls, bumps, and bruises. Contact sports and rough play must be strictly avoided.
- Avoid Intramuscular Injections: Vaccinations and medications should never be given as a shot into the muscle (e.g., flu shots). Subcutaneous or intradermal routes are preferred.
- Avoid Biopsies: Biopsying a flare-up can cause explosive new bone growth and must never be performed.
- Avoid Dental Trauma: Dental procedures should be as minimally invasive as possible. Local anesthesia without epinephrine and careful technique are crucial.
- Avoid Surgical Removal of Bone: Attempting to surgically remove heterotopic bone almost always leads to much more severe bone regrowth.
- Manage Illnesses Promptly: Viral and bacterial infections can trigger flare-ups, so they should be treated early and aggressively.
Myths and Facts About Fibrodysplasia Ossificans Progressiva (FOP)
| Myth | Fact |
|---|---|
| FOP is contagious. | FOP is a genetic disorder. You cannot catch it from someone. |
| The body turns muscle cells directly into bone cells. | The process involves inflammation and the formation of cartilage that is then replaced by bone, similar to normal skeletal formation. It occurs in soft connective tissues, not by transforming existing muscle fibers. |
| Surgery is a viable treatment to remove the extra bone. | Surgery is strongly contraindicated. Cutting out the bone causes intense trauma, triggering a massive and often worse flare-up and bone regrowth. |
| People with FOP are born with a second skeleton. | The heterotopic skeleton forms progressively after birth, usually starting in childhood. The toe malformation is the only bone abnormality present at birth. |
| There is nothing that can be done for FOP. | While there is no cure, proactive management (preventing flare-ups, medication during flare-ups, and specialized care) can significantly improve quality of life. Promising clinical trials for targeted therapies are underway. |
Treatments and Therapy
The management of FOP is primarily preventive and supportive. The goal is to minimize flare-ups and manage symptoms to preserve mobility and function for as long as possible.
Medication-Based Treatments
- Corticosteroids: High-dose corticosteroids (e.g., prednisone) are the standard of care for managing acute flare-ups in the head and neck region if started within the first 24 hours. They help reduce severe inflammation.
- Non-Steroidal Anti-Inflammatory Drugs (NSAIDs): Used for pain and inflammation management during flare-ups.
- Mast Cell Inhibitors: Medications like ketotifen are sometimes used to help stabilize the immune response and reduce flare-up frequency.
- Investigational Drugs: Several drugs targeting the overactive ACVR1 receptor (e.g., Palovarotene) and other pathways in the BMP signaling cascade are in advanced clinical trials, offering the first hope for directly slowing the disease process.
Surgical Treatments
Surgery is almost always avoided due to the high risk of provoking catastrophic new bone formation. It is only considered in life-threatening situations, such as severe jaw locking leading to malnutrition.
Physical Therapy and Rehabilitation
- Gentle Range of Motion: Passive, non-forceful movement may be recommended by a specialist to maintain joint flexibility, but it must be done with extreme care to avoid causing microtrauma.
- Assistive Devices: Occupational therapists can provide devices like long-handled reachers, adaptive utensils, and specialized chairs to help maintain independence.
Lifestyle and Behavioral Interventions
This is the cornerstone of management. It involves all the prevention strategies listed above, along with maintaining a healthy weight to reduce stress on joints and practicing excellent dental hygiene to minimize invasive procedures.
Alternative and Complementary Medicine
Some patients find relief with acupuncture (must be very superficial) or cool compresses for pain. However, any deep-tissue massage or manipulative therapy is dangerous. All such interventions must be discussed with an FOP specialist.
Psychotherapy and Counseling
Living with a progressive, disabling condition is immensely challenging. Psychological support is crucial for patients and families to cope with anxiety, depression, social isolation, and the emotional toll of the disease.
Immunizations and Vaccines
Vaccinations are critically important to prevent infections that could trigger flare-ups. However, they must be administered subcutaneously, never intramuscularly.
Stem Cell Therapy
While theoretically intriguing, stem cell therapy is not a current treatment for FOP. The challenge is that the problem is not a lack of cells, but a faulty genetic instruction given to the body’s own connective tissue stem cells.
Gene Therapy
Gene therapy—correcting or silencing the faulty ACVR1 gene—represents the ultimate hope for a cure. While research is active in laboratories, it is still in the early, preclinical stages and is not yet available for human patients.
Top 20 FAQ with Answer on Fibrodysplasia Ossificans Progressiva (FOP)
1. What exactly is FOP?
FOP is a rare genetic disorder where the body forms extra bone in muscles, tendons, and ligaments, progressively locking joints and creating a second skeleton.
2. Is FOP contagious?
No, it is a genetic condition and cannot be spread.
3. How is FOP inherited?
Most cases are from a spontaneous new mutation. An affected person has a 50% chance of passing it to their children.
4. What is the life expectancy for someone with FOP?
Life expectancy is reduced, with many individuals living into their 40s. The most common cause of death is respiratory failure due to restricted chest movement.
5. Can the extra bone be surgically removed?
No, surgery almost always causes much more aggressive and extensive bone regrowth.
6. Is there a cure for FOP?
Not yet. However, research is very active, and several drugs are in clinical trials that aim to slow or stop the progression.
7. What triggers a flare-up?
Flare-ups can be triggered by minor trauma (falls, bumps), viral illnesses, muscle fatigue, immunizations (if IM), or dental procedures. Sometimes they occur spontaneously.
8. How is FOP diagnosed?
It is primarily diagnosed by its clinical features: the characteristic malformed big toes and the history of soft-tissue swellings that turn to bone. Genetic testing can confirm the ACVR1 mutation.
9. Can people with FOP have children?
Yes, but pregnancy can be high-risk due to physical limitations and the potential for flare-ups. Genetic counseling is essential.
10. What is the most common initial symptom?
The toe malformation is present at birth. The first major symptom is often a painful neck or back lump in early childhood.
11. Does FOP affect the brain or intelligence?
No, the heterotopic bone formation does not occur in the brain or inside the skull. Intelligence is unaffected.
12. Can you feel the extra bone?
Yes, once it has matured, the heterotopic bone is hard and palpable under the skin.
13. What should you avoid if you have FOP?
Avoid all intramuscular injections, biopsies, falls and trauma, contact sports, and forceful stretching or manipulation of joints.
14. Is physical therapy safe for FOP?
Only very gentle, passive range-of-motion exercises prescribed by a therapist who specializes in FOP is safe. Aggressive physical therapy is harmful.
15. Does FOP affect the face?
Yes, heterotopic bone can form in the jaw joints, leading to difficulty opening the mouth (ankylosis), which affects eating and dental care.
16. Are there any support groups for FOP?
Yes, organizations like the International FOP Association (IFOPA) provide vital support, resources, and community for patients and families.
17. Can FOP be detected before birth?
Yes, if the genetic mutation in a family is known, prenatal genetic testing (like amniocentesis) can identify if a fetus has FOP.
18. What is the “head-to-toe” progression?
Flare-ups typically start in the neck, shoulders, and upper back during childhood, then progress down the body to the limbs and hips. The jaw is often affected later.
19. Is pain a constant feature of FOP?
No, pain is usually episodic and associated with active flare-ups. Chronic pain can occur due to joint immobility and pressure from the extra bone.
20. Where is the best place to receive care for FOP?
Care should be coordinated through a specialized clinical center with experience in FOP, such as those affiliated with the IFOPA or major research universities.
Conclusion
Fibrodysplasia Ossificans Progressiva is one of the most dramatic and disabling conditions in medicine. For centuries, it was a disease of mystery and profound hopelessness. Today, the landscape has changed dramatically. The discovery of the ACVR1 gene in 2006 unlocked the molecular secret of FOP, paving the way for targeted drug development. While a cure remains on the horizon, current management focuses on meticulous prevention of flare-ups and supportive care to optimize quality of life. The future for individuals with FOP is brighter than ever, filled with the tangible promise of effective therapies that could one day halt the process of this “second skeleton” in its tracks.
Find Trusted Cardiac Hospitals
Compare heart hospitals by city and services — all in one place.
Explore Hospitals
This guide explains Fibrodysplasia Ossificans Progressiva with great clarity and sensitivity, especially how it connects genetic mutation with progressive bone formation and daily life challenges. I appreciated the emphasis on early diagnosis, avoiding unnecessary trauma, and careful long-term management, which offers both knowledge and reassurance to readers. Informative, compassionate, and very helpful for raising awareness about this rare and complex condition